Campus updates
COVID-19 101: Q&A with Prof Ed Rybicki
06 April 2020 | Story Nadia Krige. Photo Supplied. Read time 7 min.
In times of crisis, the human imagination tends to fluctuate between two extremes: being employed as a powerful tool for survival or wielded as a toxic weapon of destruction. As the COVID-19 pandemic spreads around the globe, leaving economic and social chaos in its wake, we’ve seen countless expressions of both extremes flick across our screens.
In the case of the former, there has been a surge in solidarity as people find creative ways to encourage others, create community and spread positivity. Sadly, however, the latter seems to be present too – especially in the spread of fake news, false information and fearmongering.
In an effort to get some COVID-19 facts straight, UCT News consulted with Professor Ed Rybicki, director of the Biopharming Research Unit in the University of Cape Town’s (UCT) Department of Molecular and Cell Biology. Rybicki is a plant virologist by training, and a biotechnologist and vaccinologist by funding circumstances. He has extensive experience in molecular virology and virus diversity studies with plant and human and animal viruses, which has led to his working with a number of vaccine and expression system platforms.
This interview, the first of two, delves into frequently asked questions about COVID-19. The second interview looks specifically at the development of a possible vaccine.
Nadia Krige (NK): What is the definition of a novel virus? How do they develop? How common are novel viruses?
Ed Rybicki (ER): A novel virus is just one we haven’t seen before – and given that we have only just scratched the surface (5 000-odd characterised viruses total) of the estimated 340 000 viruses that probably infect mammals alone, they are extremely common.
One species of fruit bat alone, in Bangladesh, was found to harbour around 60 viruses. They were all from families of viruses that we know something about, but nearly all were “novel” – exactly as this SARS-CoV-2 [Severe acute respiratory syndrome coronavirus 2] (COVID-19) is.
NK: Why is COVID-19 causing so much more havoc than previous novel viruses, such as H1N1, for example?
ER: I don’t think it is in fact causing more havoc. The original H1N1 that emerged in 1918 – the so-called “Spanish Flu” – caused a lot more havoc than this virus: it killed 50 to 100 million people worldwide and infected over one-third of the estimated 1 500 million alive at the time – and it travelled around the world by ship and by train.
The “Asian” flu that emerged in 1957 – H2N2 – killed over 2 million people, at a time when the world population was only nearly 3 billion, and air travel was not nearly so common.
The H1N1 that emerged in 2009 was related both to the original 1918 virus and to circulating viruses, which included H1N1 and had adapted to mammals by circulating in pigs, so it was less virulent. It still killed 240 000 people worldwide, though.
NK: From an academic/scientific perspective, was a pandemic of this magnitude anticipated? If so, why did it catch the world so off guard?
ER: This kind of pandemic, if not one caused by this specific virus, has been predicted for many years. Organisations like the World Health Organization have been talking about preparedness for “Virus X” for years; I have been teaching students at UCT about “The Big One” for more than 30 years, although I had flu in mind. The film Contagion was based on exactly this kind of scenario – a virus popping out of a setting where wild animals are placed in proximity to domesticated ones in meat markets.
[COVID-19] apparently caught the world unawares because governments – although not infectious disease epidemiologists – simply haven’t put time, effort and money into establishing the infrastructure to deal with it.
China is in fact an exception: they had entire hospitals built as prefabricated units after the original SARS scare in 2003, in anticipation of a resurgence of SARS, and they were able to put them up and deploy them in record time. Everyone else, well, they could have watched what was happening in China and acted pre-emptively, but they simply didn’t.
Denialism of a sort, I suppose?
South Africa has actually acted far earlier and far more decisively in our epidemic than just about any country in Europe, and especially quicker than the United States.
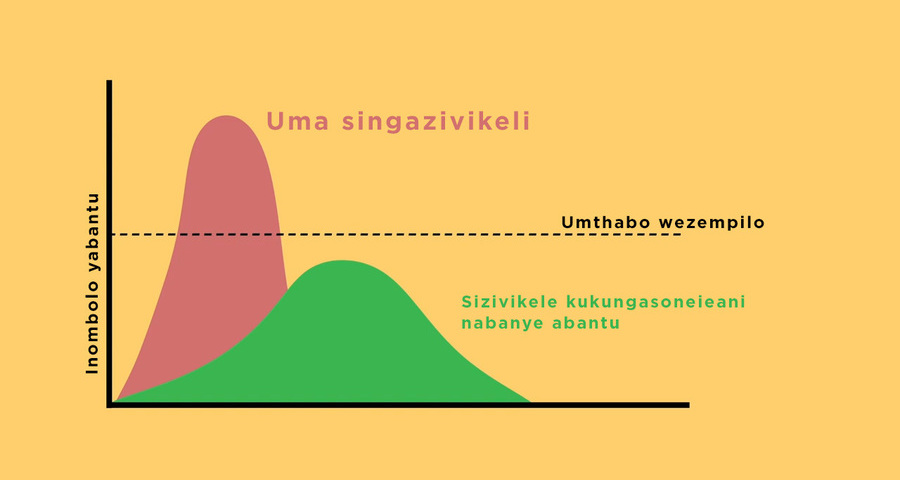
NK: Can you explain how measures like social distancing and complete lockdowns help to stem the spread of the virus, ie how does “flattening the curve” work?
ER: This article from The Washington Post actually explains it very well, with an active simulator you can play with.
What distancing and isolation does is to drastically limit the potential for spread of the virus. Instead of giving the virus to another 2.5 or so people in an uncontrolled setting, each infected person infects one or none; if the transmission rate goes below 1, the virus dies out as it is not propagated enough.
In a limited but not total lockdown scenario, the virus spread is slowed down dramatically, so that even if the same number of people get infected as would have been in an uncontrolled setting (unlikely), it happens much more slowly, and medical facilities are not overwhelmed by a huge rush of serious cases all at once, and can actually cope.
NK: I read somewhere that COVID-19 could become a seasonal occurrence (similar to the flu). Is this accurate? If so, would it become less lethal the more people have become immune/vaccinated?
ER: This is possible: several coronaviruses currently infect humans seasonally, and all cause variations of the “common cold”, along with a variety of rhinoviruses (related to polioviruses) and even adenoviruses.
Burtram Fielding from the University of the Western Cape wrote a thought-provoking piece on The Conversation recently wherein he speculated on how a supposed influenza pandemic in 1889 could have been a bovine coronavirus, which has since become a mild seasonal infection in humans.
As long as there are people still infected – and these could be asymptomatic – the virus could maintain itself in humans indefinitely. Having had it or having been vaccinated could significantly lessen this, especially for people with comorbidities.
NK: With a burgeoning world population and unprecedented movement between continents and countries, what are the chances of outbreaks like these occurring more often?
ER: Sadly, excellent. We have seen three outbreaks of betacoronaviruses alone in 17 years (SARS, MERS [Middle East respiratory syndrome-related coronavirus] and SARS-2); we had a flu pandemic in 2009; Ebola jumped out to cause two major outbreaks in West and Central Africa in four years. We can expect more, and more frequently, as human populations increasingly infringe upon wild animal habitats.
Read the second interview with Professor Rybicki for insight into the development of a vaccine for COVID-19. His blog post “Plant-made vaccines and reagents for SARS-CoV-2 in South Africa” also makes for excellent reading on a possible vaccine.
 This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Please view the republishing articles page for more information.





Coronavirus Disease 2019 updates
COVID-19 is a global pandemic that caused President Cyril Ramaphosa to declare a national disaster in South Africa on 15 March and implement a national lockdown from 26 March.
UCT is taking the threat of infection in our university community extremely seriously, and this page will be updated regularly with the latest COVID-19 information.






Daily updates
Campus communications



Resources
Video messages from the Department of Medicine
Getting credible, evidence-based, accessible information and recommendations relating to COVID-19
The Department of Medicine at the University of Cape Town and Groote Schuur Hospital, are producing educational video material for use on digital platforms and in multiple languages. The information contained in these videos is authenticated and endorsed by the team of experts based in the Department of Medicine. Many of the recommendations are based on current best evidence and are aligned to provincial, national and international guidelines. For more information on UCT’s Department of Medicine, please visit the website.









To watch more videos like these, visit the Department of Medicine’s YouTube channel.
Useful information from UCT







External resources












News and opinions















































As the COVID-19 crisis drags on and evolves, civil society groups are responding to growing and diversifying needs – just when access to resources is becoming more insecure, writes UCT’s Prof Ralph Hamann.
03 Jul 2020 - 6 min read Republished




The Covid-19 crisis has reinforced the global consequences of fragmented, inadequate and inequitable healthcare systems and the damage caused by hesitant and poorly communicated responses.
24 Jun 2020 - >10 min read Opinion










Our scientists must not practise in isolation, but be encouraged to be creative and increase our knowledge of the needs of developing economies, write Professor Mamokgethi Phakeng, vice-chancellor of UCT, and Professor Thokozani Majozi from the University of the Witwatersrand.
09 Jun 2020 - 6 min read Republished










































South Africa has been recognised globally for its success in flattening the curve, which came as a result of President Ramaphosa responding quickly to the crisis, writes Prof Alan Hirsch.
28 Apr 2020 - 6 min read Republished


































Statements and media releases
Media releases
Read more
Statements from Government
In an email to the UCT community, Vice-Chancellor Professor Mamokgethi Phakeng said:
“COVID-19, caused by the virus SARS-CoV-2, is a rapidly changing epidemic. [...] Information [...] will be updated as and when new information becomes available.”
We are continuing to monitor the situation and we will be updating the UCT community regularly – as and when there are further updates. If you are concerned or need more information, students can contact the Student Wellness Service on 021 650 5620 or 021 650 1271 (after hours), while staff can contact 021 650 5685.