Campus updates
Developing a vaccine for COVID-19
06 April 2020 | Story Nadia Krige. Photo Pexels. Read time 7 min.
As COVID-19 infection and morbidity rates increase around the globe, a number of companies and academic institutions have entered the race to develop a vaccine to protect us from the lethal virus. Creating a vaccine is, however, a complex process and could take several months, if not years.
In an effort to gain a measure of clarity around a possible COVID-19 vaccine, UCT News consulted with Professor Ed Rybicki, director of the Biopharming Research Unit (BRU) in the University of Cape Town’s (UCT) Department of Molecular and Cell Biology.
Professor Rybicki is a plant virologist by training, and a biotechnologist and vaccinologist by funding circumstances. He has extensive experience in molecular virology and virus diversity studies with plant and human and animal viruses, which led to his working with a number of vaccine and expression system platforms.
Nadia Krige (NK): There is much talk about the development of a possible vaccine for COVID-19. In the simplest terms possible, can you maybe explain how the process of developing a vaccine works? Where do scientists start the process?
Ed Rybicki (ER): There are several ways in which the process can be started – either growing up large amounts of wild-type virus and inactivating it (eg polio, hepatitis A) or selecting mutants of the virus that don’t cause disease in model animals and growing them up as attenuated live vaccines (eg yellow fever virus). Scientist can also start by purifying wild-type virus or virus adapted to cell or egg culture, killing it, and purifying components of the virus (eg flu, hepatitis B).
Taking the gene that codes for the most important protein and expressing it in a suitable cell culture system, so as to make a lot of non-infectious protein, is also a way the process can be started. This helps if it makes virus-like particles (eg human papillomaviruses [HPV], hepatitis B).
Another way to start the process of developing a vaccine is by putting the gene for the new virus into another – a safe virus already used as a vaccine or which is harmless to humans (eg human adenovirus and vaccinia virus vectors, vesicular stomatitis virus). Only Ebola vaccines like this have been released; all others are experimental.
Lastly, developing a vaccine can also start by using the gene itself as an mRNA or DNA vaccine. This is at the cutting edge of technology and, at present, only experimental.
NK: What are the different phases that the vaccine needs to go through?
ER:
Preclinical: testing in animals for toxicity and immunogenicity
Phase I: up to 80-odd not-at-risk healthy human volunteers, placebo-controlled trial, test for safety – with some readout of immunogenicity
Phase II: couple of hundred healthy volunteers, generally not at risk, placebo-controlled study on dosing and immunogenicity, which can grade into an early-stage efficacy trial if participants are exposed to natural infection (Phase IIb)
Phase III: placebo-controlled, double-blinded trial on up to thousands of at-risk volunteers, looking for efficacy or protection from infection and/or disease
NK: At what point can human trials start taking place?
ER: After thorough testing in animals and the manufacture of vaccine batches under strict clinical Good Manufacturing Practice guidelines.
It generally takes a couple of years, but can be accelerated to a couple of months for flu viruses as the process is very well established.
NK: What are the risks involved in human trials?
ER: It may not be safe. The trials may not be immunogenic enough and/or it is not sufficiently protective or exacerbates infections – one or two HIV vaccine trials were like this.
NK: When does one know that a vaccine is successful and safe for rollout to the public?
ER: Typically after it has been proven safe for use during phase three of human trials. However, when compassionate/emergency use is justified, this can also happen after extensive animal efficacy studies to shortcut the process. A good example of this is the Ebola vaccine used in West Africa and the Democratic Republic of the Congo.
One American vaccine for COVID-19 is being fast-tracked like this.
NK: How long would it take for a vaccine like this to be developed?
ER: Typically, seven to 15 years from scratch for development and testing. Development could be much quicker: several firms claim they were ready in a couple of months with products (eg mRNA and DNA vaccines).
NK: How far along in the process are researchers currently in developing a vaccine for COVID-19? Are any UCT researchers playing a role in the development?
ER: Several have been claimed already.
My group (BRU) and Professor Anna-Lise Williamson’s vaccine group’s postdoctoral fellow Emmanuel Margolin has already made a DNA vaccine candidate in an enhanced DNA expression vector patented by us. He is expressing the surface or S protein similarly to the way our groups already do for HIV-1 envelope protein in mammalian cells and in plants.
BRU’s spinout company Cape Bio Pharms is already making a portion of the S protein in plants as a reagent that is to be used in antibody detection tests and for helping another company make monoclonal antibodies to be used as therapeutics or in testing.
NK: It’s common knowledge that viruses evolve over time. Has the COVID-19 virus evolved already? What does this mean in terms of developing a vaccine, ie how long will a vaccine be relevant?
ER: SARS-CoV-2 is like SARS-CoV and MERS-CoV in being a betacoronavirus: these have big single-stranded RNA genomes – the biggest, in fact – and have evolved a more accurate enzyme (RNA-dependent RNA polymerase) to replicate it than influenza virus has, for example.
Thus, they evolve or rather mutate with every cycle of infection, but do so much more slowly than viruses like flu, which still take several years to evolve away from antibody recognition.
Several lineages of the virus have emerged since it started, but these are still very closely related to one another, show no differences in ability to cause disease, and almost certainly are not different immunogenically or in terms of eliciting an immune response.
It means a single vaccine could be good for years, unlike the case for flu.
NK: Lastly, are people who have contracted COVID-19 and recovered from it immune to it now?
ER: It is presumed so. The original SARS-CoV elicited antibodies that persist in people to this day, from 17 years ago.
Read the first interview with Professor Rybicki for answers to the most frequently asked questions regarding COVID-19. His blog post “Plant-made vaccines and reagents for SARS-CoV-2 in South Africa” also makes for excellent reading on a possible vaccine.
 This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Please view the republishing articles page for more information.





Coronavirus Disease 2019 updates
COVID-19 is a global pandemic that caused President Cyril Ramaphosa to declare a national disaster in South Africa on 15 March and implement a national lockdown from 26 March.
UCT is taking the threat of infection in our university community extremely seriously, and this page will be updated regularly with the latest COVID-19 information.






Daily updates
Campus communications



Resources
Video messages from the Department of Medicine
Getting credible, evidence-based, accessible information and recommendations relating to COVID-19
The Department of Medicine at the University of Cape Town and Groote Schuur Hospital, are producing educational video material for use on digital platforms and in multiple languages. The information contained in these videos is authenticated and endorsed by the team of experts based in the Department of Medicine. Many of the recommendations are based on current best evidence and are aligned to provincial, national and international guidelines. For more information on UCT’s Department of Medicine, please visit the website.









To watch more videos like these, visit the Department of Medicine’s YouTube channel.
Useful information from UCT







External resources












News and opinions















































As the COVID-19 crisis drags on and evolves, civil society groups are responding to growing and diversifying needs – just when access to resources is becoming more insecure, writes UCT’s Prof Ralph Hamann.
03 Jul 2020 - 6 min read Republished




The Covid-19 crisis has reinforced the global consequences of fragmented, inadequate and inequitable healthcare systems and the damage caused by hesitant and poorly communicated responses.
24 Jun 2020 - >10 min read Opinion










Our scientists must not practise in isolation, but be encouraged to be creative and increase our knowledge of the needs of developing economies, write Professor Mamokgethi Phakeng, vice-chancellor of UCT, and Professor Thokozani Majozi from the University of the Witwatersrand.
09 Jun 2020 - 6 min read Republished










































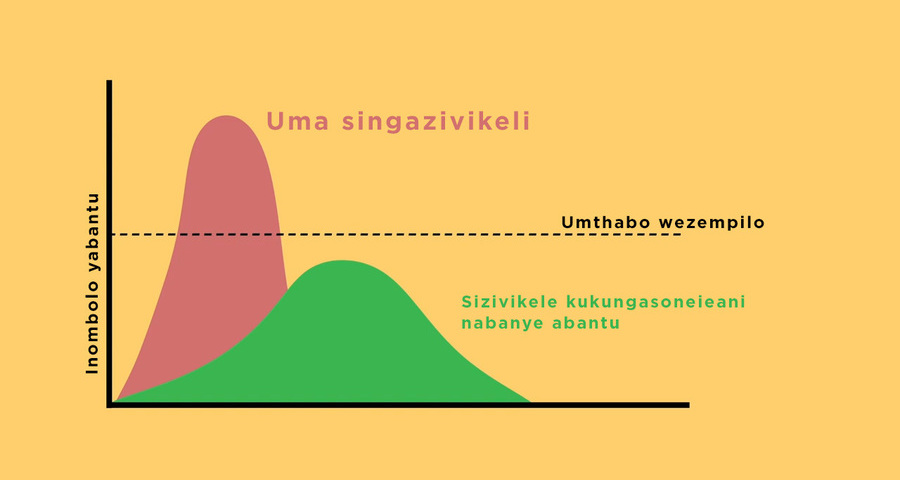
South Africa has been recognised globally for its success in flattening the curve, which came as a result of President Ramaphosa responding quickly to the crisis, writes Prof Alan Hirsch.
28 Apr 2020 - 6 min read Republished


































Statements and media releases
Media releases
Read more
Statements from Government
In an email to the UCT community, Vice-Chancellor Professor Mamokgethi Phakeng said:
“COVID-19, caused by the virus SARS-CoV-2, is a rapidly changing epidemic. [...] Information [...] will be updated as and when new information becomes available.”
We are continuing to monitor the situation and we will be updating the UCT community regularly – as and when there are further updates. If you are concerned or need more information, students can contact the Student Wellness Service on 021 650 5620 or 021 650 1271 (after hours), while staff can contact 021 650 5685.